Building bridges between cancer patients and personalized care
Dr. Monika Krzyzanowska and collaborators develop app for cancer patients to manage and understand their treatment symptoms from the comfort of their own home
Dr. Monika Krzyzanowska, Medical Oncologist at the Princess Margaret Cancer Centre
Patients undergoing cancer treatment face a lot of uncertainty. They often experience symptoms and treatment side effects at home, which often leads them to the emergency room. But in many cases, their side effects could have been better managed remotely and prevented from getting worse. Dr. Monika Krzyzanowska, Medical Oncologist at the Princess Margaret Cancer Centre, wanted a better option for her patients to understand and manage their symptoms comfortably at home.
“Almost half of women undergoing treatment for breast cancer visit the emergency room between treatment sessions and many of these visits can be avoided,” says Krzyzanowska. “We give our patients a lot of information up front, but we can do a better job at remote monitoring and providing them with the information they need when they need it. There’s a clear need for decision aids, self-management support, improved communication and options in care delivery.”
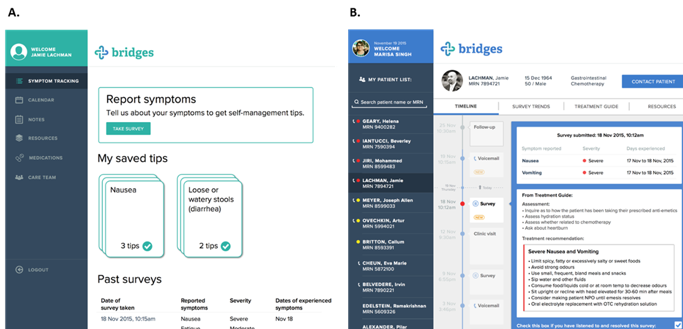
Krzyzanowska teamed up with the University Health Network’s Healthcare Human Factors team to explore how to improve symptom management for patients with a more personalized approach. In response to this need, they created bridges, a web-based app to facilitate remote management of chemotherapy-related side effects.
As recently described in the Journal of Medical Internet Research, the team refined their design over two rounds of usability testing with patients. They incorporated toxicity tracking, self-management advice and health care provider communication functionalities so that both physicians and patients can track and manage the patient’s symptoms.
Screenshots of the bridges app from the patient/caregiver (left) and health care provider (right) user interfaces.
With their pilot complete, Krzyzanowska is looking to partner with health care providers and decision makers to expand the project and explore how to integrate bridges into current systems and processes.
“Bringing bridges into the hands of patients is going to require a coordinated effort between decision makers, patients, care providers and hospitals,” says Krzyzanowska. “Helping patients who need it when they need it is our top priority and I look forward to developing bridges to help in that goal.”
Krzyzanowska’s project is one of the many research projects funded through OICR and Cancer Care Ontario’s Health Services Research Network.
What could we do if we had a clearer picture of prostate cancer?
OICR-supported trial finds new, more sensitive imaging technique can inform treatment decisions and benefit those with recurring prostate cancer
Prostate cancer is the most common type of cancer found in men, but managing the disease is difficult because not all prostate cancers are aggressive and overtreatment can lead to unnecessary side effects, such as hormone imbalances, bowel function issues and erectile dysfunction. After initial treatment, prostate cancer patients are often monitored with a prostate specific antigen (PSA) blood test, but this test provides no information about the location and the extent of the disease. Even with traditional bone scans and CT scans, remnant traces of the disease are difficult to find and often go undetected.
Dr. Glenn Bauman, Radiation Oncologist and Chief/Chair of the Department of Oncology at the London Health Sciences Centre and lead of the PICs study.
A few years ago, a new, more sensitive type of imaging technique had shown promise in early clinical studies abroad and Dr. Glenn Bauman, Radiation Oncologist at the London Health Sciences Centre, wanted to bring this technique into his practice. He recognized the potential benefits of this method, but didn’t realize how much it could impact the lives of his patients.
Bringing advances to local patients
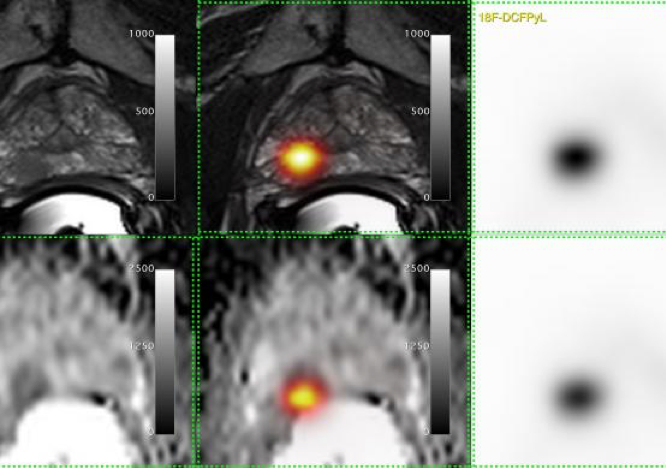
The new technique, which was originally developed at the John Hopkins Hospital in Baltimore, consisted of a chemical probe, called [18-F]-DCFPyL, which would attach only to prostate cancer cells and light up in positron emission tomography (PET) scans. It can detect very small traces of a tumour that has returned after treatment or spread to a different part of the body.
Bauman teamed up with the co-inventor of [18-F]-DCFPyL, Dr. Martin Pomper, and the Centre for Probe Development and Commercialization (CPDC) to bring this probe to patients in Ontario. CPDC implemented the stringent manufacturing processes needed to create this probe and in March of 2016, Lawson’s researchers were the first to use this technique to scan a patient at St. Joseph’s Hospital in London.
A copy of the first [18-F]-DCFPyL PET/MRI (top) and PET/CT images (bottom) captured in Canada. (Photo: Lawson Health Research Institute)
“We teamed up with experts in [18-F]-DCFPyL from the U.S. and experts in prostate PET/CT from Australia to adopt this new technique, benchmark our methods and learn from their experience,” says Bauman. “It’s with collaborations like these that we can accelerate the implementation of new methods to help patients in Ontario.”
Evaluating the benefits for those with prostate cancer
Clinical studies are needed to evaluate the effectiveness new medical techniques in practice. For this technique, Bauman and collaborators needed to test whether it’s improved accuracy and sensitivity could help make better treatment decisions.
“Treatment plans for prostate cancer differ depending on the cancer’s size and location. Whether a cancer returns in the prostate, the pelvic area or elsewhere makes a big difference,” says Bauman. “We needed to test if more sensitive imaging techniques could help patients make better treatment decisions.”
Bauman led the design and development of the Advanced Prostate Imaging of Recurrent Cancer After Radiotherapy (PICs) study to evaluate [18-F]-DCFPyL PET/CT imaging. With OICR’s support over the following two years, PICs enrolled 80 men and scanned them with both traditional imaging methods and with [18-F]-DCFPyL PET/CT.
The study group found that not only can [18-F]-DCFPyL PET/CT detect smaller traces of the disease earlier when it is more manageable, this technique changed treatment recommendations for two in every five patients.
“With this technique, we were able to clarify and reclassify a lot of the traditional scans that were previously uncertain,” says Bauman. “This means that we were able to give prostate-directed treatment with confidence for patients whose cancers reemerged in their prostate and avoid the negative side effects of systemic hormone therapy for these patients.”
Bauman says that the technique also detected double the number of cancers outside of the prostate which were too small to be detected using traditional imaging alone.
Translating clinical findings into practice
Just three years after the first [18-F]-DCFPyL PET/CT scan was taken in Canada, Bauman has embarked on the next stage in translating these findings into routine practice. He and collaborators have teamed up with Cancer Care Ontario to provide access to the [18-F]-DCFPyL PET/CT technique in Toronto, London, Hamilton, Ottawa and Thunder Bay as part of a provincial registry program.
[18-F]-DCFPyL PET/CT can be applied to other challenges that patients and clinicans face with managing prostate cancer, including monitoring how patients respond to treatments. Notably, investigators in Hamilton are investigating how these scans can help predict a patient’s response to treatment in the OICR-supported MISTR trial.
“We have been sufficiently encouraged by our results from the PICs study, through which we have demonstrated the value of this intervention and how it can benefit men with prostate cancer,” says Bauman. “I’m proud to help bring better technologies to our patients in need and enable the adoption of these technologies throughout the province.”
An innovative way to look at genome rearrangements leads to new insights about ovarian cancer
Dr. Paul Krzyzanowski, Director of Genome Technology Translation at OICR.
Researchers look beyond an obvious hypothesis to connect patterns in gene expression with genome rearrangements, drawing attention to often-overlooked regions of the genome
If two different genes come together, the resulting gene fusion can have a new function that can cause or contribute to cancer. The discovery of cancer-causing gene fusions has led to the development of new therapies for many cancer types and sparked efforts to identify rearrangements that might yield new treatment targets. Often, however, researchers discover fusions with no effect on a cell, but a recent study has shown that the regions around these ‘fusions of unknown significance’ may be just as important to study as the fusion itself.
In their investigation into high grade serous ovarian cancer (HGSOC) – which has a five-year survival rate of only 20 per cent – the Genomics Program at OICR identified thousands of gene fusions and investigated the regions around these key points. As described in Scientific Reports, they found that the neighbouring regions are overexpressed – in essence, overactive – which may contribute to the cancerous nature of cells.
“Often, we find evidence of rearranged DNA without a clear picture of how rearrangements drive cancer,” says Dr. Paul Krzyzanowski, Director of Genome Technology Translation at OICR and primary author of the publication. “In this study, we found that the regions around gene fusions – in addition to the fusions themselves – are very active in cancer cells. This observation hints at the idea that we can look at broader genetic regions, and not just the location of a fusion by itself, to better understand how genomic rearrangements wreak havoc in cancer cells.”
In this study, we found that the regions around gene fusions – in addition to the fusions themselves – are very active in cancer cells
The observed overexpression of regions around fusions could be used to differentiate diseased cells from normal cells and lead to new cancer treatment approaches. The observations in this study are consistent with findings from the Pan-Cancer Analysis of Whole Genomes network, which identified patterns of overexpression in disturbed genomic regions across many cancer types.
Krzyzanowski says this work highlights a non-intuitive analytical approach for analyzing cancer-related gene fusions which will continue to be employed as OICR’s Ovarian Cancer Translational Research Initiative investigates how DNA rearrangements in ovarian cells drive cancer.
Read more about OICR’s Ovarian Cancer Translational Research Initiative or learn more about Genomics at OICR.
The unanticipated early origins of childhood brain cancer
Study identifies earliest traces of brain cancer long before the disease becomes symptomatic
Toronto (May 1, 2019) – Brain tumours are the leading cause of non-accidental death in children in Canada, but little is known about when these tumours form or how they develop. Researchers have recently identified the cells that are thought to give rise to certain brain tumours in children and discovered that these cells first appear in the embryonic stage of a mammal’s development – far earlier than they had expected.
Their findings, published today in Nature, could lead the way to the discovery of better treatments to attack these lethal tumours.
“Progress in the
development of more effective brain cancer treatments has been hampered in
large part by the complex heterogeneity – or the variety of cells – within each
tumour,” says Dr. Michael Taylor, Paediatric Neurosurgeon and Senior Scientist
in Developmental and Stem Cell Biology at The Hospital for Sick Children (SickKids)
and co-lead of the study. “We recognized that new technologies could allow us
to unravel some of this complexity, so we combined our expertise with McGill
and OICR to approach this problem together.”
Using mouse models, the
research group investigated the different types of normal brain cells and how
they developed at various timepoints in the cerebellum of the brain – the most
common location for childhood brain tumours to appear. They mapped the lineages
of over 30 types of cells and identified normal cells that would later transform
into cancerous cells, also known as the cells of origin.
To pinpoint these
specific cells, the group relied on single cell sequencing technology, which
allows researchers to look at individual cells more clearly than traditional
sequencing methods.
In their investigation, the cells of origin were observed much earlier in fetal development than one would expect, says Taylor, who is also a Professor in the Departments of Surgery and Laboratory Medicine and Pathology at the University of Toronto and Co-lead of OICR’s Brain Cancer Translational Research Initiative.
“Our data show that in
some cases, these tumours arise from cell populations and events that would occur
in humans at six weeks in utero,” says Dr. Lincoln Stein, Head of Adaptive
Oncology at OICR and co-lead of the study. “This means that the brain tumours
may be starting long before they show in clinic, even before a woman may know
she is pregnant.”
“The brain is extraordinarily complex. These findings are not only important for better understanding brain tumours but they will also allow us to learn more about these cells and how they work, in order to help children with neurodevelopmental delays. What we have accomplished as a team in this study brings hope for patients,” adds Dr. Nada Jabado, Paediatric Hemato-Oncologist and Senior Scientist in the Child Health and Human Development Program at the Research Institute of the McGill University Health Centre and co-lead of the study. Dr. Jabado is also a professor of Pediatrics and Human genetics at McGill University.
“If
we can understand where these tumours originate, we can better understand which
cells to target and when to target them to create more effective and less toxic
therapies for children,” says Ibrahim El-Hamamy, PhD candidate at OICR and
co-first author of the study. “We’ve found new avenues and opportunities in a
very complex disease and we look forward to actualizing this potential.”
With this knowledge, researchers can now study the differences between the development of normal, healthy cells and the cells that will eventually give rise to cancerous cells.
Targeting fat production could help tackle leukemia
Collaborative research group discovers a key pathway in the development of acute myeloid leukemia – and a potential new therapeutic strategy to treat the disease
Dr. Mingjing Xu and Ayesh Seneviratne pose in the Schimmer Lab at the University of Toronto.
Despite
progress in the treatment of acute myeloid leukemia (AML), many patients still
die from relapse or experience significant side effects from treatment. Dr.
Aaron Schimmer, who is Research Director of the Princess
Margaret Cancer Centre and co-lead of OICR’s Acute Leukemia Translational
Research Initiative, worked with his
collaborators to understand the root cause of AML relapse to develop more effective
and less toxic therapies. Their recent findings are both surprising and
promising.
The
group, which consists of researchers from across Ontario and abroad,
investigated the pathways that are uniquely important to the growth and
development of leukemic stem cells (LSCs) – also known as the cells at the
“root” of the disease. They discovered a key pathway, as described in Cell Stem Cell, which can be altered to control how LSCs mature.
Interestingly, they found that this process can be modulated with an essential
phospholipid (a type of fat), called phosphatidylserine.
“We discovered a pathway that these stem cells rely on. We investigated further and found that interfering with lipid metabolism – that is, the fats within these cells – could potentially slow their growth and reduce their ability to cause relapse,” says Ayesh Seneviratne, MD/PhD candidate in the Schimmer Lab at the University of Toronto and co-first author of the publication.
Normally, phosphatidylserine
is important in maintaining the integrity of the cell membrane and normal cell
function, but the authors found that within LSCs, phosphatidylserine acted as a
trigger for the cell to lose its self-renewal properties. They are the first
group to describe increasing phosphatidylserine as a potential therapeutic
strategy for AML.
“We now better understand
the function of this metabolite in leukemia, and in turn, we have found a new way
to target the disease,” says Dr. Mingjing Xu, postdoctoral fellow in the
Schimmer Lab and co-first author of the publication. “We are enthusiastic to
pursue further studies and unravel how phosphatidylserine ceases leukemia
growth.”
Schimmer says that this work
could not have been done without the contributions of many collaborators.
“This discovery is a product
of a concerted effort between many researchers,” says Schimmer. “Together, we’ve
found new insights into the biology of leukemia and turned those insights into
a new potential therapeutic strategy.”
Advancement in nanopore sequencing opens new areas of cancer biology to exploration
Dr. Jared Simpson, OICR Investigator.
OICR’s
Dr. Jared Simpson and collaborators at the University of Oxford create a new method
that allows researchers to explore the fundamental, but hard-to-study biological
process of DNA replication
How DNA replicates in a cancer cell is difficult
to understand, in large part due to the limitations of current technologies. Nanopore
sequencing – a fast, portable way to read very long molecules of DNA – could allow
researchers to detect DNA replication patterns. Experts in DNA replication from
Oxford University, led by Drs. Carolin Müller, Michael Boemo and Conrad
Nieduszynski, teamed up with OICR’s expert in nanopore sequencing, Dr. Jared
Simpson, to tackle this challenge.
Together, they developed D-NAscent, a
sophisticated laboratory protocol and computational tool that together allow
researchers to detect and study how DNA is replicated. Recently, the group’s techniques
were published in Nature
Methods.
“Traditional methods of studying DNA
replication have limited resolution – how finely we can see these patterns,”
says Simpson, an Investigator at OICR, who helped develop the computational
methods used in the study. “With our methods, we can now look at DNA
replication on individual, long molecules of DNA at high throughput. This gives
us the ability to look for biological patterns that we were once unable to see,
for example, in repetitive areas of the genome.”
The collaborators built on the methods
that were previously developed by Simpson et
al. which have allowed the researchers to study epigenetic changes in
cancers and track
other diseases like Ebola.
In the study published today, the group used their
methods to study yeast cells, which have a simpler and smaller genome than
human cells. Now, the group will apply D-NAscent to study the DNA replication
dynamics of human cancer biology. They’ve released their software
freely to allow other researchers to do so as well.
“We’re very excited to apply D-NAscent in human
cancer cells,” says Simpson. “The potential of this technology is what excites
me. We’ve opened up an entirely new way to look at genomic diseases – one that
can potentially turn an unexplored aspect of biology into new cancer research
discoveries.”
OICR welcomes new Principal Investigator, Dr. Sagi Abelson
Dr. Sagi Abelson, OICR Principal Investigator.
OICR is proud to welcome Dr. Sagi Abelson to its
Computational Biology Program as a Principal Investigator. Here, Abelson
discusses some of his past successes, including his recent
leukemia research and his wide range of research
interests.
How have you been involved with OICR in the past?
I came to Toronto and joined Dr. John Dick’s
lab at the Princess Margaret Cancer Centre as a Postdoctoral Fellow, where I
had the opportunity to work with OICR’s Genomics and Genome Sequence
Informatics teams. I was investigating the differences between normal aging cells
and the cells that lead to leukemia. To do that, we had to look into blood-derived
DNA samples from many individuals that develop leukemia following blood
collection and search for common genetic markers that indicated a high risk of
developing leukemia. I worked closely with OICR teams to prepare and sequence these
patient samples. We also collaborated to deploy specialized methodology that
enabled us to accurately interpret the genomic data and to identify those harmful
mutations.
What motivated you to become involved with that subject?
Far too many patients are diagnosed with
leukemia when it is too late. This applies to many other cancers as well. If we
can detect a disease earlier, we may benefit from a larger window of
opportunity to prevent, manage, or treat the disease. There are many biological
and computational challenges that need to be addressed in this area, including
finding extremely small traces of a disease amidst a lot of noise in genomic
data. I’m interested in the development and the optimization of methods and computational
tools to find these first traces of a developing disease.
What will your future research focus on?
In the future I would like to expand my
research program to other types of cancers. I truly believe that as a researcher
I can achieve more by having a multidisciplinary team that address questions in
other biological systems as well. In this era of big data, we are not the only
ones realizing that multiple research skills are necessary to tackle the toughest
problems. Research institutes and universities understand it as well and
therefore introduced computational courses in their biology curricula. That
said, conducting research is a team effort and collaboration is the key to
approaching scientific problems in areas where you don’t have the expertise.
When approaching the end of your postdoctoral studies and
deciding the next step in your career, what opportunities were you considering?
Well, I was looking for a combination of
things. I was looking for a place that shares the same vision as I do, the same
values of collaboration and translation and a place that has a high caliber of
scientists. I believe in the things that OICR works on and how research is done
here, so I think it’s a great fit.
What advice would you give to aspiring academics?
To do research well, you first need to love it.
You need to be curious, know to identify the needs and ask the right question
at the right time. Furthermore, you have to have persistence. You cannot give
up in the pursuit of new knowledge.
Unraveling the circuitry behind brain cancer
Collaborative research group identifies new cancer-driving mechanisms in brain cancer stem cells, describes novel ways to overcome the limited effectiveness of standard therapy
Dr. Graham MacLeod works at a lab bench at the University of Toronto.
Glioblastoma is the most common and the most deadly type of brain cancer found in adults, yet there have been no new advances in treating this disease for almost two decades. Recent research has provided a wealth of knowledge about the genomics – or the abnormal genetic code – of glioblastoma, but this has yet to translate into new treatments for patients. Understanding which genes drive glioblastoma can help uncover new ways to treat this incurable disease, and a pan-Canadian research group has set out to do just that.
Researchers from the University of Toronto, The Hospital for Sick Children and the University of Calgary have teamed up to identify genetic vulnerabilities in brain cancer stem cells – the cells that often resist treatment and cause the disease to return in patients after treatment. Their recent findings, which were published today in Cell Reports, uncovered new targets for glioblastoma and unraveled some of the complex mechanisms behind the disease.
Dr. Graham MacLeod
“We set out to understand which genes are important functionally,” says Dr. Graham MacLeod, co-primary author of the study and Research Associate in the lab of Dr. Stéphane Angers at the University of Toronto. “Connecting a gene to its function is a bit like connecting circuits on a very complex circuit board. If we can understand which genes are important, then we can find hints into where to unplug, plug in, stop and start mechanisms so that we can potentially stop the progression of the disease.”
The group used CRISPR-Cas9 gene editing tools, which Angers and MacLeod specialize in, to investigate all 20,000 genes within the genome and identify the key genes that are required for glioblastoma cells to survive and grow. In their study, they identified one gene in particular whose function is already targeted in leukemia treatments. Angers says this is promising “because it uncovered a biological process, not previously suspected to be implicated in glioblastoma, for which a small molecule drug already exists.”
As part of OICR’s Brain Cancer Translational Research Initiative, the next stage of their research will use the same gene editing approach to investigate tumour cells after therapy to find the genes or the genomic changes that help tumour cells evade treatment and recur in patients.
Researchers work to save lives by improving follow-up of colorectal cancer screening tests
Research group identifies the nuanced barriers that prevent patients from following up on a positive colorectal cancer screening test
Colorectal cancer (CRC) is often detectable and
beatable, yet it still remains the second leading cause of cancer-related death
in Canada. Ontario offers an at-home CRC screening test, however not all
patients who have abnormal test results receive the necessary follow-up care
due to a number of factors. This means that there are missed opportunities to treat
– and cure – some of these cancers.
Dr. Jill Tinmouth at the Sunnybrook Research
Institute has set out to improve follow-up after a positive CRC screening test.
The first step, Tinmouth says, is to understand why patients may be reluctant
to follow up in the first place.
Dr. Jill Tinmouth
“The screening test for colorectal cancer is an
easy, safe, painless, at-home fecal occult blood test (FOBT) but without proper
follow-up of abnormal tests, it is all for naught,” says Tinmouth. The FOBT
checks a person’s stool for tiny drops of blood, which can be caused by CRC. Colonoscopy
is the recommended next step for anyone who has an abnormal FOBT. “Looking at
the administrative data, we saw that nearly one in three people with an
abnormal FOBT don’t follow up with colonoscopy within six months. We are
working to both understand and fix this gap.”
In this first study, Tinmouth and collaborators looked into Ontario’s administrative
health data to try to improve the lack of follow-up. These
initial findings suggested that physicians may not be adhering to screening
guidelines and led to better articulation of CRC screening and follow-up protocols
to primary care providers.
“We made some modifications to our screening
program to encourage physicians to follow up on positive FOBT results in a
timely manner, but we recognized that these strategies wouldn’t solve every
problem,” says Tinmouth. “To fully understand the gaps and barriers to
following up, we knew we had to speak directly to patients and those in this
position.”
In their most recent study on the subject,
published in the American Journal
of Gastroenterology, Tinmouth teamed up with Dr. Diego Llovet from
Cancer Care Ontario to interview patients who failed to follow-up on positive
FOBT results and physicians who care for those patients. Many of the patients
believed that their test results were a false positive and others experienced
fear, anxiety or uneasiness about the next step in CRC screening – a colonoscopy.
Often, patients were reluctant to have a colonoscopy and physicians were unable
to persuade their patients to follow through.
Tinmouth is now working with health system decision-makers and Cancer Care Ontario to test and pilot four different interventions that could help improve proper follow-up, including patient navigation through the screening process and reminders sent to physicians of patients who test positive but fail to follow up. This research group is evaluating the feasibility of these interventions and how Ontario could implement them across the province.
“Better colon cancer screening and care starts with understanding the barriers and then effectively implementing this new knowledge,” says Tinmouth. “On these projects, researchers worked hand-in-hand with policy-makers – in so doing, we were able to integrate our expertise and collective wisdom to improve colorectal cancer screening for Ontarians today and in the future.”
The winner of last year’s FACIT Falcons’ Fortunes pitch competition is already seeing early success in moving her product to the clinic
The winner will soon meet with U.S. regulators, marking a major step towards commercializing her innovative polymer product, ReFilx™, and bringing it to breast cancer patients.
Dr. David O’Neill, President, FACIT, and Dr. Soror Sharifpoor, Co-Founder and Chief Executive Officer, Polumiros Inc., pose for a photo.
It took only 10 minutes for a panel of investors and industry experts to recognize that Dr. Soror Sharifpoor and her oncology product – ReFilx™ – were worth supporting. Last spring, she pitched ReFilx™ in the FACIT Falcons’ Fortunes competition and won the top prize – the $50,000 Ernsting Entrepreneurship Award. Almost 12 months later, Sharifpoor and her team at Polumiros Inc. will be meeting with the U.S. Food and Drug Administration (FDA) to officially begin the regulatory submission process – a necessary first step in bringing their product to patients.
ReFilx™ is a polymer designed to fill the breast tissue cavities left in breast cancer patients following a lumpectomy. The polymer dissolves over time, allowing the patient’s cells and tissue to regrow in its space, thus preventing breast tissue defects from forming.
“ReFilx™ could improve the emotional and mental well-being of breast cancer patients,” says Sharifpoor. “In addition to the psychosocial benefits, it could also encourage surgeons to take more aggressive margins around the tumour, thereby reducing the chances of cancer recurrence.”
Bringing ReFilx™ to the clinic requires rigorous clinical testing and regulatory review, which begins with a pre-submission meeting with the FDA. FACIT’s support allowed Sharifpoor to continue with pre-clinical testing, hire a regulatory consultant and further develop ReFilx™ into an injectable form.
In a few months, Sharifpoor and her team will have the pre-submission meeting to collect feedback on their product, which will then be used to guide their future submission to the FDA and their plans for further clinical research. Polumiros Inc. intends to pursue this research in Canada.
“We’re excited to initiate our regulatory submission process,” says Sharifpoor. “We’re fortunate to have had FACIT’s support, allowing us to develop ReFilx™ faster and smarter than we would have on our own.”
FACIT, OICR’s strategic partner in commercialization, is hosting its 6th annual pitch competition this year on April 4, 2019. The Falcons’ Fortunes event will feature six aspiring entrepreneurs from across the province who are developing oncology-related innovations. FACIT runs the annual competition as part of its broader mandate to support translation of cancer research to benefit Ontario’s economy and patients worldwide.
This website uses cookies in order to optimize the user’s experience. To learn more about how we use cookies on this website, please review our Website Privacy Statement. Your browser settings may allow you to turn off cookies. By continuing to use our website site without changing your browser settings, you consent to our use of cookies in accordance with Website Privacy Statement
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
Other uncategorized cookies are those that are being analyzed and have not been classified into a category as yet.
This website uses cookies in order to optimize the user’s experience. To learn more about how we use cookies on this website, please review our Website Privacy Statement. Your browser settings may allow you to turn off cookies. By continuing to use our website site without changing your browser settings, you consent to our use of cookies in accordance with Website Privacy Statement